By Taryn McFadden
“It’s all in your head.” Few phrases frustrate people who are in pain more, because it sounds like blame disguised as explanation. Though pain is processed in the brain, that doesn’t make it fake, imagined, or any less serious. Patients often describe something intensely real and deeply personal, while clinicians seek to determine whether the pain comes from the body, the mind, or both. These different perspectives can create tension between patient and physician, causing clinical pain conversations to go wrong.1
A Model Born from Frustration
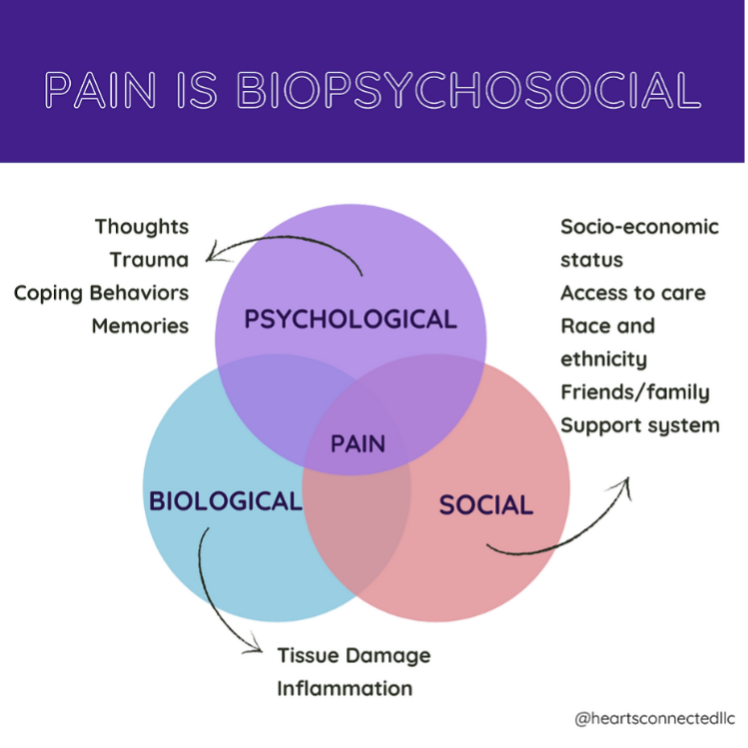
The BioPsychoSocial (BPS) model of pain offers a framework for physicians to better understand patient pain (Figure 1). Rather than locating pain in the body or the mind, the BPS model treats pain as the product of biological signals, emotional state, and life context working together.2,3
For most of modern medicine, the dominant disease framework has been the biomedical model: identify a biological cause, target it with treatment, and measure success by whether the pathology resolves. The biomedical model transformed medicine, helping to eradicate infectious diseases and dramatically extend life expectancy; however, the biomedical model is not without its flaws.4 As psychiatrist George Engel argued in his landmark 1977 article in the journal Science, the biomedical model “leaves no room within its framework for the social, psychological, and behavioral dimensions of illness”. 5 Engel proposed the BPS model as an alternative, drawing on early 20th-century Austrian biologist and philosopher Ludwig von Bertalanffy’s General Systems Theory (GST). The GST model itself was a revolutionary paradigm shift from reductionist science, where components were considered in isolation. Instead, GST proposes that intercomponent dynamics are just as noteworthy and that the whole is greater than the sum of its parts.6 Accordingly, Engel argued that health emerges from dynamic interactions among biological processes, psychological states, and social conditions. Psychological and social factors are now understood to heavily contribute to biological pain processing. In fact, these three aspects produce what systems theorists call emergent properties, or new products formed by bidirectional three-way interactions that shape health and illness in their own right.7
Why Pain Needs a New Model
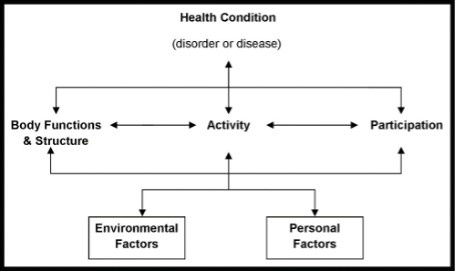
Since its psychiatric origin, the BPS model now forms the basis of the WHO’s International Classification of Functioning (Figure 2) and has since been adopted across clinical fields, including specialized chronic pain management, rehabilitation, and diabetes or aging-related care.8,9 However, despite nearly five decades of evidence supporting its validity and WHO recognition, the BPS model has had limited influence on how most healthcare is organized and funded.9 Healthcare systems remain largely designed around acute biomedical care, and the BPS model is still rarely taught as a formal framework in medical training. The lack of implementation of the BPS model matters most where the biomedical model fails, most evident in the case of chronic pain.
Pain is one of the most common reasons adults seek medical care.10 An estimated 20.9% of U.S. adults, or roughly 51.6 million people, experience chronic pain, and 6.9% (17.1 million) experience high-impact chronic pain that substantially limits essential independent daily activities.11 More recent data suggest these numbers are rising: chronic pain prevalence increased from 20.5% in 2019 to 24.3% in 2023, with higher chronic pain prevalence among women, older adults, those living in poverty, rural residents, and military veterans.10,11,12 Racial and ethnic disparities are well documented: Native American and multiracial adults report the highest pain prevalence, while Black patients are systematically undertreated for pain relative to White patients.13,14 The CDC’s 2022 opioid prescribing guideline notes that disparities persist even after adjusting for access, patient preferences, and clinical appropriateness, and that “differentially untreated or undertreated pain as a result of clinician biases persists and demands immediate and sustained attention and action”. 15 These numbers demonstrate that a model that reduces pain to only what shows up on a scan or lab test is too narrow for the scale and complexity of the pain experience.
The BPS Model: Three Dimensions of Pain
Instead of asking only what is broken in the body, the BPS model asks how biology, psychology, and social context interact to shape pain. It recognizes that pain and disability result from multidimensional, dynamic interactions among these three domains and that each domain can both cause and be changed by pain.10
Bio(logical): What causes pain?
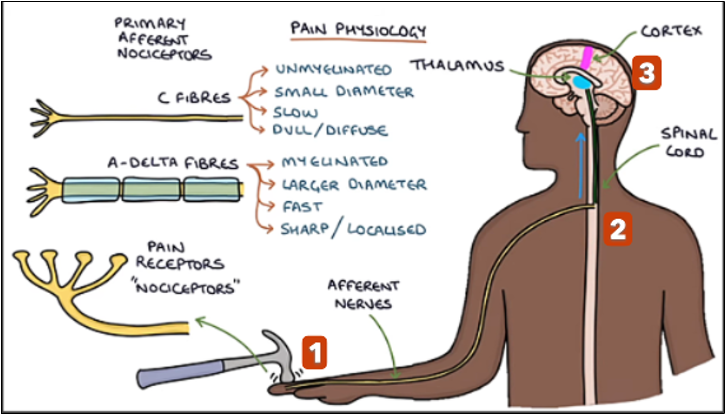
The sensation of pain starts in the body. 1) Specialized nerve endings called nociceptors detect potentially harmful changes (i.e. extreme temperature, pressure, or tissue damage) and send signals along sensory afferent nerve fibers to 2) the spinal cord and 3) the brain (Figure 3). The two primary types of nociceptors are fast, myelinated Aδ‑fibers that carry sharp, immediate pain, and slower, unmyelinated C‑fibers that carry dull, aching pain (Figure 3).16-18 Along the way, regions of the brain such as the thalamus can amplify or dampen the signal before reaching higher brain areas like the cortex.19 Some biological contributors to pain processing include genetics, age, sex, and sleep quality.10
Psycho(logical): Central sensitization of Pain
In acute pain, the pain response system works as designed: injury triggers an alarm, you protect the area from further injury, and the pain fades with healing. Chronic pain is different. Through a process called central sensitization, the central nervous system (CNS) becomes more reactive over time (Figure 4). Spinal neurons become hyperexcitable, amplifying incoming signals, making them fire more easily, while the brain’s descending inhibitory pathways, its usual “brakes” on pain, become less effective.20 The result changes psychological pain dimensions through allodynia, or pain that occurs with normally non-painful stimuli, and hyperalgesia, pain that is amplified more than expected. 21
Another side-effect from central sensitization is that it alters how pain interacts with brain systems involved in attention, mood, and threat detection.18 Chronic pain “trains” the nervous system to treat too many signals as danger, leading the person to be exhausted, anxious, or on edge.16,22 Psychological contributors to chronic pain also include depression, anxiety, post-traumatic stress, catastrophizing, and unhelpful coping patterns.10 In other words, a body in chronic pain is not weak; it is overprotective.
Social: How Context Shapes the Pain Experience
Because experience shapes the CNS, two people with identical injuries can have vastly different pain experiences. Past trauma, current stress, fear of reinjury, and whether the person feels believed all change how the nervous system processes danger.23 Some people live with nervous systems taxed by repeated physical and emotional injuries, and those systems may react more strongly to new pain signals.15 In addition to past experiences, the BPS model considers social contributors, including education, culture, social support, financial stress, access to care, and experiences of discrimination or trauma.10 The link between adversity and pain is one reason Trauma-Informed Care (TIC), an approach that recognizes how past adversity shapes present health and future outcomes, is increasingly seen as essential to effective pain management. 24
The BPS Model in Practice
The BPS model gives patients and clinicians a shared language and validates the patient’s pain experience. One in five American adults lives with chronic pain, and pain is one of the most common reasons people seek medical care.11Proper diagnosis and treatment for patients must recognize that pain is influenced by the body, the mind, and the social world.25 For clinicians, using the BPS model means asking different questions: How is pain affecting sleep? What does this person fear most? Do they have support? What trauma or stress might be keeping the nervous system on alert? Asking these questions with sensitivity, and being prepared to act on the answers, is at the heart of the BPS model. For scientists and pain researchers, the goal should be to better understand how tissue damage, the brain, the environment, and lived experience interact to explain pain more clearly and to treat pain more effectively without losing sight of the person experiencing it. Perhaps the most important takeaway is this: if your pain has been minimized because “the scan shows nothing,” that doesn’t mean nothing is wrong. It means the tools and models being used are too small for the size of your experience. The BPS model offers a way to expand those tools, moving beyond a one-size-fits-all, scan-and-prescribe mindset and toward care that is multidisciplinary, patient-centered, and can help the body and the mind.
TL; DR:
- Pain is shaped by the brain, body, emotions, and life context.
- The biomedical model of pain has significant disparities by race, gender, and socioeconomic status.
- The biopsychosocial model integrates the biological, psychological, and social dimensions of pain.
Reference
- Meints SM, Edwards RR. Evaluating psychosocial contributions to chronic pain outcomes. Prog Neuropsychopharmacol Biol Psychiatry. Dec 20 2018;87(Pt B):168-182. doi:10.1016/j.pnpbp.2018.01.017
- Hadjistavropoulos T, Craig KD, Duck S, et al. A biopsychosocial formulation of pain communication. Psychol Bull. Nov 2011;137(6):910-939. doi:10.1037/a0023876
- Duncan G. Mind-Body Dualism and the Biopsychosocial Model of Pain: What Did Descartes Really Say? Journal of Medicine and Philosophy. 2000/08/01 2000;25(4):485-513. doi:10.1076/0360-5310(200008)25:4;1-A;FT485
- Crimmins EM. Lifespan and Healthspan: Past, Present, and Promise. Gerontologist. Dec 2015;55(6):901-11. doi:10.1093/geront/gnv130
- Engel GL. The need for a new medical model: a challenge for biomedicine. Science. Apr 8 1977;196(4286):129-36. doi:10.1126/science.847460
- Drack M, Pouvreau D. On the history of Ludwig von Bertalanffy’s “General Systemology”, and on its relationship to cybernetics – part III: convergences and divergences. Int J Gen Syst. Jul 4 2015;44(5):523-571. doi:10.1080/03081079.2014.1000642
- C. Menon JC, Kumar RK, Pati S. Reframing clinical research frameworks: Case for a shift from a biomedical to a biopsychosocial one. The Indian Journal of Medical Research. 2026-03-28 2026;163:341-344. doi:10.25259/ijmr_2598_2025
- Keady J, Jones L, Ward R, et al. Introducing the bio-psycho-social-physical model of dementia through a collective case study design. Journal of Clinical Nursing. 2013/10/01 2013;22(19-20):2768-2777. doi:https://doi.org/10.1111/j.1365-2702.2012.04292.x
- Wade DT, Halligan PW. The biopsychosocial model of illness: a model whose time has come. Clin Rehabil. Aug 2017;31(8):995-1004. doi:10.1177/0269215517709890
- Cohen SP, Vase L, Hooten WM. Chronic pain: an update on burden, best practices, and new advances. Lancet. May 29 2021;397(10289):2082-2097. doi:10.1016/s0140-6736(21)00393-7
- Rikard SM, Strahan AE, Schmit KM, Guy GP. Chronic Pain Among Adults — United States, 2019–2021. MMWR Morbidity and Mortality Weekly Report. 2023-04-14 2023;72(15):379-385. doi:10.15585/mmwr.mm7215a1
- Ray M. Prevalence, burden, and factors associated with chronic pain and high-impact chronic pain in U.S. Adults, 2019-2023. J Pain. May 5 2026;45:106311. doi:10.1016/j.jpain.2026.106311
- Zajacova A, Grol-Prokopczyk H, Fillingim R. Beyond Black vs White: racial/ethnic disparities in chronic pain including Hispanic, Asian, Native American, and multiracial US adults. Pain. Sep 1 2022;163(9):1688-1699. doi:10.1097/j.pain.0000000000002574
- Hoffman KM, Trawalter S, Axt JR, Oliver MN. Racial bias in pain assessment and treatment recommendations, and false beliefs about biological differences between blacks and whites. Proceedings of the National Academy of Sciences. 2016/04/19 2016;113(16):4296-4301. doi:10.1073/pnas.1516047113
- Dowell D, Ragan KR, Jones CM, Baldwin GT, Chou R. CDC Clinical Practice Guideline for Prescribing Opioids for Pain<b>—</b>United States, 2022. MMWR Recommendations and Reports. 2022-11-04 2022;71(3):1-95. doi:10.15585/mmwr.rr7103a1
- Neugebauer V. Amygdala physiology in pain. Handb Behav Neurosci. 2020;26:101-113. doi:10.1016/b978-0-12-815134-1.00004-0
- Simons LE, Moulton EA, Linnman C, Carpino E, Becerra L, Borsook D. The human amygdala and pain: evidence from neuroimaging. Hum Brain Mapp. Feb 2014;35(2):527-38. doi:10.1002/hbm.22199
- Yang S, Chang MC. Chronic Pain: Structural and Functional Changes in Brain Structures and Associated Negative Affective States. Int J Mol Sci. Jun 26 2019;20(13)doi:10.3390/ijms20133130
- Garland EL. Pain processing in the human nervous system: a selective review of nociceptive and biobehavioral pathways. Prim Care. Sep 2012;39(3):561-71. doi:10.1016/j.pop.2012.06.013
- Volcheck MM, Graham SM, Fleming KC, Mohabbat AB, Luedtke CA. Central sensitization, chronic pain, and other symptoms: Better understanding, better management. Cleveland Clinic Journal of Medicine. 2023;90(4):245. doi:10.3949/ccjm.90a.22019
- Tomašević-Todorović S, Spasojević T. CENTRAL SENSITIZATION IN PATIENTS WITH CHRONIC MUSCULOSKELETAL PAIN. Acta Clin Croat. Nov 2023;62(Suppl4):102-106. doi:10.20471/acc.2023.62.s4.15
- Zharova N, Zharikov Y, Pelicer-Marques Y, et al. Amygdala-centered mechanisms of pain amplification and chronification in fibromyalgia and migraine: Narrative review. Behavioural Brain Research. 2026/04/12/ 2026;503:116071. doi:https://doi.org/10.1016/j.bbr.2026.116071
- Declercq J. Talking about chronic pain: Misalignment in discussions of the body, mind and social aspects in pain clinic consultations. Health (London). May 2023;27(3):378-397. doi:10.1177/13634593211032875
- Goldstein E, Chokshi B, Melendez-Torres GJ, Rios A, Jelley M, Lewis-O’Connor A. Effectiveness of Trauma-Informed Care Implementation in Health Care Settings: Systematic Review of Reviews and Realist Synthesis. Perm J. Mar 15 2024;28(1):135-150. doi:10.7812/tpp/23.127
- Craig KD, Versloot J. Psychosocial perspectives on chronic pain. Clinical Pain Management. 2022:40-49.
