By Emily Haar
Six years have passed since the World Health Organization (WHO) declared the initial COVID-19 outbreak a pandemic, and daily life came to a screeching halt across the globe. Despite the return to normalcy in more recent years, many individuals are still living with long-term consequences of this disease, especially those who have suffered from a condition known as post-COVID-19 sequelae, aka “Long COVID.” As defined by the WHO, Long COVID is a chronic condition associated with the SARS-CoV-2 virus which appears after infection, lasts at least three months, and affects more than one organ system.1 Patients tend to report neurological symptoms—including fatigue, headache, dizziness, and cognitive dysfunction—that interfere with their quality of life and ability to return to work.1,2 Notably, Long COVID can precede the onset of a neurological condition known as Postural Orthostatic Tachycardia Syndrome (POTS).
POTS can be tricky to understand—even for experts. POTS is a type of dysautonomia, meaning it impacts the autonomic nervous system, which is the part of the nervous system that regulates involuntary functions such as heart rate, breathing, and digestion. Although the name “Postural Orthostatic Tachycardia Syndrome” may seem intimidating at first, it is actually quite informative when dissected. The word “postural” relates to the position of one’s body, while the term “orthostatic” specifically refers to an upright standing position. “Tachycardia” is a fast heart rate, defined clinically as greater than 100 beats per minute. Finally, “syndrome” signifies a collection of symptoms, rather than just one. Indeed, individuals who suffer from POTS experience abnormally increased heart rate when standing up, often accompanied by feelings of lightheadedness or even fainting.3 Elevated heart rate is not the only symptom of POTS; on the contrary, POTS can affect almost every organ system in the body.4
Never heard of POTS? There might be a reason.
Person-to-person variability in people suffering from POTS has historically made it difficult for patients to receive a timely diagnosis. However, POTS is starting to receive more recognition due to increased cases following the COVID-19 pandemic. Mayo Clinic physicians first described the syndrome in 1993, but as recently as 2019, over two-thirds of providers admitted to having never heard of it.4,5 Many who have tend to view it as an “uncommon” condition; however, it has been estimated that that roughly 1% of the population has POTS—more than neurological conditions known by the general population, such as multiple sclerosis and Parkinson’s disease.3,4 This number may even be an underestimate, as POTS often goes undiagnosed.
POTS misdiagnosis happens for a few reasons. Firstly, the lack of awareness means that providers do not even consider POTS as an option when patients come to them with symptoms. Besides increased heart rate while standing, symptoms include chest discomfort, shortness of breath, nausea, constipation, diarrhea, abdominal pain, and peripheral acrocyanosis, which is a bluish color in the extremities due to insufficient oxygen levels3,5. Often, symptoms such as dizziness, headache, fatigue, and a type of cognitive dysfunction known as “brain fog” get misinterpreted as psychological in nature. In fact, 83% of patients report that they were misdiagnosed with a psychiatric condition.4 Because of these challenges, patients on average see seven providers across six years before being properly diagnosed.4 These delays are incredibly frustrating, and many patients have described the experience of finally being diagnosed with POTS as “life changing”.5
Gender bias may also play a role in misdiagnosis. POTS affects four to five women for every one man, and typically occurs in women of childbearing age.3–5 Nevertheless, the diagnostic delay for women is 7.0 years—almost twice as long as the 3.8-year delay experienced by men.5 Women are also far more likely than men to have their symptoms be misattributed to anxiety and to be put on a mental healthcare plan.5 In reality, male and female POTS patients have similar rates of anxiety and health-seeking behavior, which suggests that the drastic differences in diagnostic delays may be related to clinician bias, rather than patient behavior.5
So, what causes POTS, anyway?
Experts have not identified a singular cause for POTS. Instead, POTS is thought to be a “final common pathway” that emerges from dysfunction in multiple processes.3 When healthy individuals stand up, the force of gravity shifts blood from the chest to the lower extremities, which causes a decrease in blood pressure that makes it harder for the veins to return blood to the heart.4 The autonomic nervous system detects this change and signals a corrective response. Part of this response is an increase in heartbeat to maintain blood flow while veins in lower extremities tighten to increase blood pressure. Once blood pressure is stabilized, heart rate returns to normal. In healthy individuals, this should occur within seconds. In individuals with POTS, the autonomic response is insufficient, and the heart continues to beat faster than normal. Most of the time in POTS patients, this elevated heart rate maintains blood flow to the brain and other organs, but insufficient blood flow can sometimes lead to lightheadedness and eventual fainting.
What’s COVID got to do with it?
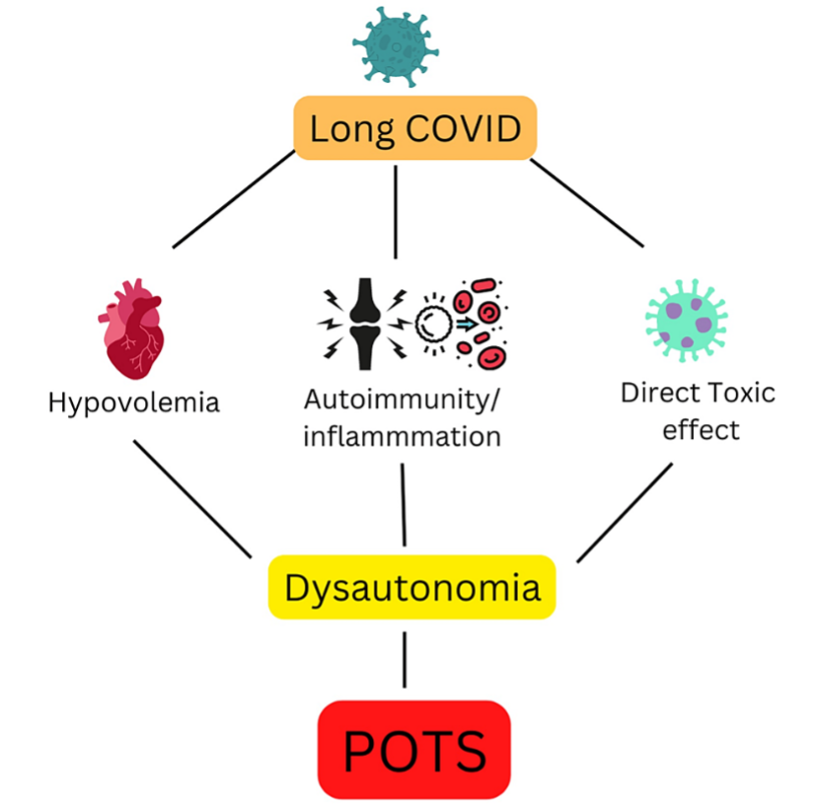
Since the COVID-19 pandemic, reported POTS cases have increased, and the connection between POTS and Long COVID in particular was identified in 2021.1,2 The exact mechanism behind this phenomenon is still unknown, but experts have proposed multiple hypotheses (Figure 1).6 Firstly, COVID-19 infection can lead to a low volume of circulating blood known as hypovolemia, which is a common underlying cause of POTS.6 Hypovolemic individuals have a smaller volume of blood circulating throughout their body compared to their healthy counterparts, so their hearts must pump blood faster when standing in order to maintain adequate blood flow throughout the body. Secondly, COVID-19 infection may also lead to autoimmunity—a condition in which the immune system fails to distinguish between “self” and “non-self” properly and attacks healthy cells.6 In some patients who develop autoimmunity in response to COVID-19, the immune system attacks parts of the autonomic nervous system responsible for the constriction of blood vessels needed to return blood to the heart.6 Consequently, the heart must beat faster to maintain appropriate blood flow upon standing. Moreover, it is unclear whether there is something unique about POTS related to COVID-19, or if such cases are just another example of POTS triggered by a viral infection.2,6 The American Autonomic Society has introduced the diagnosis of Long COVID-19 POTS (LC-POTS), which occurs when POTS symptoms last for at least twelve weeks following infection.2 Compared to patients whose POTS is unrelated to COVID-19, the population of LC-POTS patients tends to be slightly older and less skewed towards female patients.2 Although the exact number of LC-POTS cases is not known, studies estimate that about 15 to 33% of Long COVID patients develop LC-POTS.7 These are only rough estimates because 1) many Long COVID and POTS symptoms overlap with each other, 2) LC-POTS diagnoses can rely too heavily on symptom questionnaires, and 3) the reported frequency of LC-POTS cases varies from study to study.2
A study published in late 2025 seems to have clarified some of the uncertainty surrounding LC-POTS1. The connection between POTS and Long COVID had already been found before this study; however, the frequency of POTS diagnosis within the Long COVID population remained unknown at this point due to variations across studies. Moreover, differences in both the physical and mental health of Long COVID patients who developed POTS compared to Long COVID patients who did not develop POTS were not well understood. The researchers addressed both knowledge gaps in their experimental design.
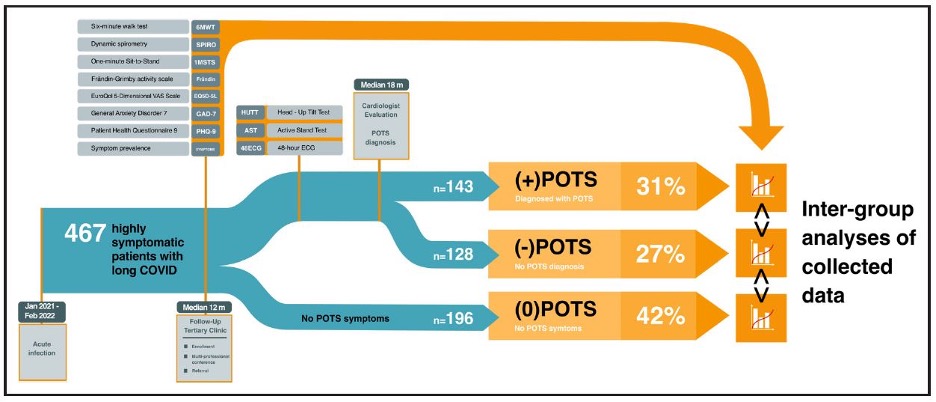
To address the question of LC-POTS frequency reliably, this study included a cohort of 467 highly symptomatic patients with Long COVID, making it much more robust than previous work.1 A sample size of this magnitude is no easy feat. For starters, patients with missing data (i.e., due to missed study visits or human error) must be excluded from analysis.1 Though a common roadblock in clinical research, enrollment across the entire study was especially relevant here, given that POTS symptoms can fluctuate. Follow-up specialist visits were therefore crucial to ensure POTS diagnoses were not missed due to low symptom presentations on a specific day. Patients referred to a post-COVID outpatient clinic in Stockholm, Sweden were eligible for this study. To be included, patients needed to meet strict criteria: at least 18 years of age, at least 12 weeks of COVID-19 symptoms, a clinical evaluation to confirm Long COVID diagnosis, and a follow-up clinical evaluation. Out of the total 467 patients, the 271 who presented clinical signs of POTS were referred to a cardiologist for diagnostic confirmation based on 1) an increase in heartbeat of at least 30 beats per minute upon standing up, 2) at least three months of symptoms, and 3) no other causative conditions. About half of those referred were confirmed to have POTS (Figure 2). POTS was confirmed in one-third of the total cohort, which is much greater than the estimated 1% in the general population. Out of those who were referred to a cardiologist, symptom prevalence—even cardiac symptoms—were similar between those who were diagnosed with POTS and those who were not. Importantly, these results support the idea that providers should not use symptoms alone to diagnose LC-POTS but rather tests in which heart rate is measured before and after standing up.
In addition to the correlation between Long Covid and POTS, this study demonstrated how LC-POTS negatively impacted patients’ quality of life. Participants self-reported physical activity levels both before and after Long COVID, and all three groups reported levels indicative of an active lifestyle.1 However, after Long COVID, the individuals diagnosed with POTS reported significantly lower physical activity than individuals with no POTS symptoms. Moreover, individuals with POTS walked a shorter distance compared to the other individuals, even those with POTS symptoms and no diagnosis, in a Six-Minute Walk Test (6MWT). During the 6MWT, the individuals with POTS also had a significantly higher heart rate, as well as a greater change in absolute heart rate. These results suggested that LC-POTS negatively impacted patients’ physiological functions. Interestingly, history of psychiatric illness in the cohort was within the range seen in the rest of the Swedish population, pointing to LC-POTS being physiological in nature rather than psychological.
Although the onset of the COVID-19 pandemic may feel like a distant memory for most, the long-term consequences of the virus have yet to be fully unraveled, as evidenced by the unsolved puzzle of LC-POTS. Scientific progress is slow, but steady. For one, development of Long COVID and POTS both occur over months, so studying LC-POTS requires patience. Large sample sizes enhance the rigor and reproducibility of findings, but the trade-off for robust research is time. Nevertheless, such research is necessary, as it can provide insight into how quality of life can be worsened by these chronic conditions. The study described here, and hopefully future research on LC-POTS, will prove to be invaluable contributions to our understanding of how COVID-19 continues to affect our lives, even years post-pandemic.
TL; DR:
- One consequence of “Long COVID” can be the development of Postural Orthostatic Tachycardia Syndrome (POTS).
- Patients with Long COVID develop POTS at a much higher rate than the general population, the causes of which are physical not psychological.
Reference
- Björnson, M. et al. Prevalence and Clinical Impact of Postural Orthostatic Tachycardia Syndrome in Highly Symptomatic Long COVID. Circ. Arrhythm. Electrophysiol. 18, (2025).
- Tavee, J. Current concepts in long COVID-19 brain fog and postural orthostatic tachycardia syndrome. Ann. Allergy. Asthma. Immunol. 133, 522–530 (2024).
- Arnold, A. C., Ng, J. & Raj, S. R. Postural tachycardia syndrome – Diagnosis, physiology, and prognosis. Auton. Neurosci. 215, 3–11 (2018).
- George, A. & Winters, B. Postural Orthostatic Tachycardia Syndrome (POTS): A Frequently Missed Diagnosis. J. Nurse Pract. 19, 104439 (2023).
- Lau, D. H. et al. Postural Orthostatic Tachycardia Syndrome: A State-of-the-Art Review. Heart Lung Circ. 35, 171–185 (2026).
- Mallick, D. et al. COVID-19 Induced Postural Orthostatic Tachycardia Syndrome (POTS): A Review. Cureus https://doi.org/10.7759/cureus.36955 (2023) doi:10.7759/cureus.36955.
- Hira, R., Karalasingham, K., Baker, J. R. & Raj, S. R. Autonomic Manifestations of Long-COVID Syndrome. Curr. Neurol. Neurosci. Rep. 23, 881–892 (2023).
