By Stephanie Baringer
In recent years, the process in which therapeutics are approved for use by the FDA has been in the spotlight. From the emergency use of COVID-19 vaccines (read more in a previous LTS article) to the approval of then-anticipated breakthrough drug aducanumab for Alzheimer’s disease (see my previous LTS article on the topic), there are a lot of questions surrounding the approval process. Why do some therapeutics need accelerated approval? Is an accelerated approval as safe? What does the future hold for the process?
It is no secret that it takes ages for a therapeutic to make it to market and at the bedside of patients in need. On average, the entire clinical trial pipeline – from phase 1 to FDA approval – takes about 9 years (see my previous LTS article on the topic). This timeline varies based on the patient population and the therapeutic in testing. For example, studies that use survival or cognitive benefit over time as primary endpoints (such as oncology or neurology therapeutics respectively) can last for significantly longer amounts of time because it simply takes more time to ensure clinical benefit1. Additionally, therapeutics developed to deliver unmet needs to rare disease populations are challenged with recruiting enough participants to produce meaningful results2. Without a little regulatory ‘push’ these patient populations would have to wait even longer for potentially life-saving therapeutics, which is why the FDA created the accelerated approval process – not to be confused with the emergency authorization use that COVID-19 vaccines employed to obtain approval.
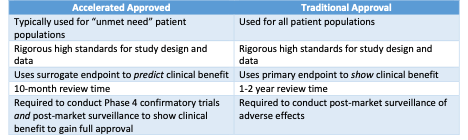
In the 1980s, HIV and AIDS were ravaging communities in the United States. In response to the crisis and desperate need for treatment options, the FDA created the Accelerate Approval Program3. Therapeutics available on the market through accelerated approval are held to the same high standards as therapeutics accepted through the traditional approval route. The key difference is the endpoint measurement. Traditional approved therapeutics are required to have a primary endpoint to show clinical benefit. Accelerated approvals use a surrogate endpoint, which is a measurable result that can likely predict clinical benefit, otherwise known as a biomarker4. Many criticize the use of surrogate endpoints, especially when published research is conflicting or absent on the endpoint’s proven causal relationship with clinical benefits5, look no further than the dichotomy between amyloid-β reduction and cognitive benefit in Alzheimer’s disease trials. For that reason, once granted accelerated approval, therapeutics must undergo phase 4 trials within a specific timeline (as outlined by the FDA) to confirm the predicted clinical benefits4. Another factor that speeds up the accelerated approval timeline is the review priority at the FDA4. Therapeutics in the pipeline are given top priority and jump to the front of the metaphorical line, allowing reviewers to pour over the data for the same amount of time as they normally would to determine if the therapeutic in question is safe and effective. All in all, nearly 300 therapeutics have been approved through the accelerated pathway since its creation, with only 9% of them rescinded6.
One example of accelerated approval pathway use is teclistamab for the treatment of relapsed or refractory multiple myeloma (RRMM) patients. Multiple myeloma is a cancer of plasma cells (an immune cell found within bone marrow) with about 35,000 new cases each year in the United States and a median survival rate of 6 to 9 months7. While there are successful treatments for multiple myeloma, 84% of patients experience recurrence of the cancer, which then does not respond to the same therapies as before8. This initial responsiveness to treatment followed by resistance is what classifies RRMM. Teclistamab, developed by Janssen Pharmaceuticals, is a first-in-class bispecific antibody that aims to deliver an unmet need to this patient population by targeting B-cell maturation antigen and CD3, which are exclusive to plasma cells and universally expressed in multiple myeloma9. Teclistamab was granted accelerated approval by the FDA on October 25, 2022 based on a phase 2 clinical trial that showed an overall response rate of 62% and the median overall survival of participants was increased to 18.3 months10. The surrogate endpoint used to gain approval was the overall response rate as classified by a decrease of cancerous plasma cells. Teclistamab was listed on Clarivate’s Drugs to Watch list of 2023 due to its projected market growth of $1.8 billion in 2031.
The future of the FDA’s Accelerated Approval Program is currently playing out in real time. In December 2022 the Food and Drug Omnibus Reform Act was passed to resolve issues with phase 4 confirmatory studies for accelerated therapeutics11. Prior to the reform, the FDA held little legislative power to require companies to conduct their promised post-approval trials to confirm clinical benefit. Additionally, if the trials failed to show clinical benefit, the process for the FDA to remove the therapeutic from the market was time consuming and ineffective. A report from the Office of Inspector general for the Department of Health and Human Services found that approximately 42% of outstanding confirmatory studies took more than a year post-approval to get started or had not started at all12. The new law gives the FDA more leverage to hold companies accountable. Specifically, it allows the FDA to require initiation of confirmatory trials at the time of filing for approval and it removes some bureaucratic red tape that slowed down market removal in the case of no clinical benefit12.
Accelerated approvals are still far from perfect, but there is no denying their utility in allowing beneficial therapeutics getting to patients in need. Teclistamab is expected to benefit the approximately 72,000 patients living with multiple myeloma. At the end of the day, improving patient outcomes is the driving force of biomedical research at the bench, in clinical trials, and on the desk of an FDA reviewer.
TL:DR
- The FDA Accelerated Approval Program allows therapeutics that deliver an unmet need to be fast tracked for approval based on predicted clinical benefit
- About 300 therapeutics have been granted accelerated approval
- A new law gives the FDA more power to enforce post-approval studies to confirm clinical benefit
References:
1. How long a new drug takes to go through clinical trials. Cancer Research UK https://www.cancerresearchuk.org/about-cancer/find-a-clinical-trial/how-clinical-trials-are-planned-and-organised/how-long-it-takes-for-a-new-drug-to-go-through-clinical-trials (2014).
2. Mellerio, J. E. The challenges of clinical trials in rare diseases. British Journal of Dermatology 187, 453–454 (2022).
3. Research, C. for D. E. and. Accelerated Approval Program. FDA https://www.fda.gov/drugs/nda-and-bla-approvals/accelerated-approval-program (2023).
4. FDA Accelerated Approval. EveryLife Foundation for Rare Diseases https://everylifefoundation.org/accelerated-approval/.
5. Weintraub, W. S., Lüscher, T. F. & Pocock, S. The perils of surrogate endpoints. Eur Heart J 36, 2212–2218 (2015).
6. Novack, G. D. Expedited regulatory product approval in the time of COVID-19. Ocul Surf 26, 345–348 (2022).
7. What Is Multiple Myeloma? https://www.cancer.org/cancer/multiple-myeloma/about/what-is-multiple-myeloma.html.
8. Multiple Myeloma Relapse: Rate, Treatment and Life Expectancy. Cancer Treatment Centers of America https://www.cancercenter.com/cancer-types/multiple-myeloma/types/relapsed-multiple-myeloma (2022).
9. Moreau, P. et al. Teclistamab in Relapsed or Refractory Multiple Myeloma. N Engl J Med 387, 495–505 (2022).
10. Research, C. for D. E. and. FDA approves teclistamab-cqyv for relapsed or refractory multiple myeloma. FDA (2022).
11. Rep. Eshoo, A. G. [D-C.-18. H.R.7667 – 117th Congress (2021-2022): Food and Drug Amendments of 2022. http://www.congress.gov/ (2022).
12. Lupkin, S. FDA has new leverage over companies looking for a quicker drug approval. NPR https://www.npr.org/sections/health-shots/2023/03/03/1160702899/fda-enforcement-drug-approval-manufacturer-promises (2023).
