By: Lina Jamis, 1st year student in the Anatomy Graduate Program
 Anybody who knows me knows that I love a good read. So when I picked up a bright yellow book entitled Brain on Fire, in late 2012, it wasn’t a surprise that I devoured it in the course of a single afternoon.
Anybody who knows me knows that I love a good read. So when I picked up a bright yellow book entitled Brain on Fire, in late 2012, it wasn’t a surprise that I devoured it in the course of a single afternoon.
Brain on Fire is the firsthand account of New York Post reporter Susannah Cahalan’s “lost month of madness,” pieced together by an imperfect memory of the events surrounding her hospitalization and descent into madness—the result of what became a rather surprising diagnosis.
Cahalan’s story begins in 2009 when she began to exhibit strange symptoms; she became obsessed with bedbugs, developed numbing migraines and tingling in her left hand, became emotionally unstable, and had persistent insomnia and paranoia. Then came the first of many seizures.

Susannah Cahalan
At this point, Cahalan was hospitalized at NYU and thus began a more frantic quest for accurate diagnosis. Because she was a flight risk and subject to seizures, she was constantly under video surveillance. These videos and accounts of her parents and boyfriend became the only memory she had of this period. One thing was certain from all of these outside perspectives: she was not herself—not by a long shot.
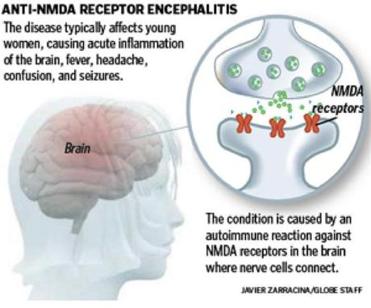
After a slew of physicians and psychiatrists failed to diagnose her (one neurologist even suggesting that she had been partying too hard), Cahalan’s path crossed a physician by the name of Souhel Najjar, who suspected that she might be suffering from anti-NMDA receptor encephalitis. A brain biopsy confirmed his suspicions, making Cahalan the 217th person worldwide to receive this diagnosis. “It just begged the question. If it took so long for one of the best hospitals in the world to get to this step, how many other people were going untreated, diagnosed with a mental illness or condemned to a life in a nursing home or psychiatric ward?”
Normally, the cells that make up the body’s immune system have the ability to distinguish an infectious agent from parts that are identified as ‘body’ but sometimes the immune system is fooled into attacking its own healthy parts. Some of the most dramatic examples are the resulting neuroimmunologic disorders that arise from an inflammatory attack in the central nervous system.
This is nothing new, however. After all, multiple sclerosis is an autoimmune disorder that is caused by inflammatory attack on the myelin of axons of the central nervous system. But anti-NMDA receptor encephalitis is different—the autoimmune system specifically attacks NMDA receptors, the most prominent glutamate receptor in the nervous system. These receptors control various cognitive functions, mood, behavior, personality traits. When compromised, a whole host of neurological symptoms surface. It is also the same receptor that is blocked by PCP or ketamine, both of which can make a normal individual appear schizophrenic.
 What causes the disease? That’s not entirely clear. But as with other autoimmune disorders, a genetic predisposition may contribute to an individual’s risk.
What causes the disease? That’s not entirely clear. But as with other autoimmune disorders, a genetic predisposition may contribute to an individual’s risk.
Bizarrely, a recent study from the University of Pennsylvania found that up to 55% of female patients under 18 years of age who had anti-NMDA receptor encephalitis also had teratomas in their ovaries—a finding that also held true for Cahalan.
Josep Dalmau, the physician who originally reported anti-NMDA receptor encephalitis, first noticed that female patients with a history of teratomas also appeared to have behavioral and personality changes that had evolved into severe neurological impairment. Armed with their blood and spinal fluid Dalmau exposed slices of rat brains to the affected women’s spinal fluid. Extraction and isolation of the rat brains showed similar patterns of reactivity: antibodies bound to the NMDA receptors, which were presumably produced in response to the teratomas.
By 2007, Dalmau gave the disease a name: anti-NMDA receptor encephalitis. But more questions were raised: how were these antibodies gaining access to the brain? And how could these individuals be treated? While the first question is still unknown, Cahalan received intravenous immunoglobulin, an inflammation suppressant, to fight off her body’s exaggerated immune response. The treatment was successful.
 Calahan’s experience begs the question: how many people are walking around with a psychiatric diagnosis and being treated with psychotropic drugs, but may, in fact, have a potentially curable auto-immune disease? This question might change the way in which psychiatrists first approach patients with new-onset psychosis and how we diagnose those who find themselves suddenly burdened with psychiatric symptoms.
Calahan’s experience begs the question: how many people are walking around with a psychiatric diagnosis and being treated with psychotropic drugs, but may, in fact, have a potentially curable auto-immune disease? This question might change the way in which psychiatrists first approach patients with new-onset psychosis and how we diagnose those who find themselves suddenly burdened with psychiatric symptoms.
Either way, it is lucky that Cahalan recovered so quickly and with such fortitude to go on and recount her story to those who couldn’t possibly understand what it might be like to lose our minds and our bodies. And Cahalan’s story has a happy ending—she still writes at the New York Post and has made a full recovery—but the epic odyssey that she endured from bedbugs to recovery is powerfully real and powerfully scary.
