By: Andrew Huhn, 4th year PhD candidate in the Neuroscience Graduate Program

Image: Adam from UK (Wikimedia Commons)
Americans are abusing prescription painkillers at an alarming rate.
In 2012, 259 million prescriptions were written for opioid analgesics – that’s enough for every adult in the U.S. to have their own bottle of pills, according to the Centers for Disease Control. Opioid analgesics are a class of drug that includes Vicodin, Percocet, and OxyContin; it’s quite likely that you or a family member has been prescribed one of these after having surgery.
In addition to providing pain relief, opioid analgesics also activate the brain’s reward system, making it easy to become addicted. Given their similar mechanism of action, prescription opioid use can lead to heroin use. After all, heroin has become significantly less expensive and doesn’t require a doctor’s prescription.
While the current heroin boom is getting a lot of press, prescription opiate addiction gets little attention even though it leads to more overdose deaths per year than heroin and cocaine combined.
But can you fix an addiction to pills…with a pill?

Image: Baker131313 (Wikimedia Commons)
Opiate addiction is a progressive disease marked by physical and psychological dependence, as well as chronic relapse. Initially, opiates instill intense feelings of euphoria. As opiate use continues, addicts end up taking more pills for diminishing effect; this is called “tolerance.” At the same time, cravings become incredibly intense, making it difficult for opiate addicts to stop the cycle. Staying off the drug is another matter entirely, as cravings do not go away following withdrawal.
Many recovering addicts have found coping mechanisms to deal with these cravings in 12-step meetings. In fact, there is evidence to support that the 12-step philosophy is most effective in changing behaviors given its focus on the person rather than the drug. Unfortunately, in many cases, it can be hard for a recovering addict to be receptive to group therapy.
The medical profession has long been in search of a “cure,” or at least a treatment that effectively curbs cravings and behaviors associated with addiction. There have been several pharmacotherapies developed, and although the efficacy of these therapies is frequently hailed by doctors, people in recovery are often wary of their usefulness and potential side effects.
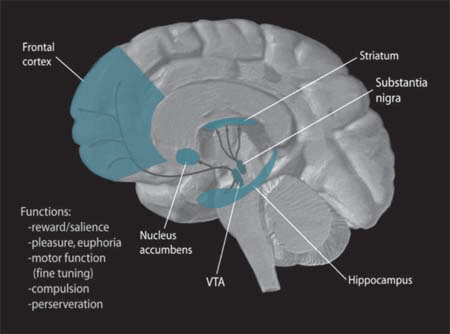
The brain’s reward pathway, shown in blue. Image: NIDA (Wikimedia Commons)
Of the plethora of treatment options for addiction, many health care professionals are getting behind a class of drugs called Mu opioid receptor antagonists.
Mu opioid receptors are thought to be the primary mediators of opiate addiction because of their influence over the brain’s reward system (the part of the brain that underlies all addiction). Drugs that antagonize a receptor essentially block the effect of the receptor; in this case, the ability of opiates to activate the reward system is blocked.
Mu opioid receptor antagonists include naltrexone (taken once daily) or Vivitrol (a long-acting version of naltrexone that is given via injection once a month). The drug’s effect can be overridden, but there is a much greater risk of overdose in people trying to get high while on naltrexone. In addition, these drugs are thought to cut down on cravings, making the addict less likely to want to relapse.
Image: Mahamaya1 (Wikimedia Commons)
Of course, like any drug, there are side effects to using naltrexone, including gastrointestinal problems (diarrhea or constipation), anxiety, and joint/muscle aches, to name a few. When deciding on treatment options for an individual, one should consider whether the side effects outweigh the benefits.This is the trickiest part of treating addiction, and the answer may change on an individual basis.
But there is an even larger, more philosophical question to consider: is it even a good idea to treat addiction to one pill by prescribing another pill? Doesn’t this keep the addict dependent on a substance?
Roger E. Meyer, M.D., Penn State College of Medicine addiction psychiatrist and author of The Heroin Stimulus, thinks naltrexone can be a helpful tool “only when paired with outpatient treatment.”
For instance, if someone is receiving outpatient treatment (likely after a stay in a residential facility), and there is a trained doctor overseeing its use, naltrexone might be a good option for 3-6 months. He goes on to say that “the drug is not the answer.” The idea is that, in combination with outpatient therapy, it may tip the scale in the patient’s favor and help them achieve a period of abstinence that they can build on.

Image: NCI (Wikimedia Commons)
Unfortunately, some physicians keep their patients on naltrexone (or Vivitrol) for years at a time, or indefinitely. While it may be seen as the lesser of two evils, there is no study that has examined the long-term effects of opioid antagonists. These drugs aren’t meant to be a cure, but rather a crutch to be used in the early (and often hardest) stage of recovery.
While some “12-step purists” would caution against any pharmacotherapy, it seems prudent to at least consider using an antagonist like naltrexone if the patient is struggling. After all, there are still physiological responses to drug cues long after a recovering addict goes through withdrawal.
No matter your opinion on addiction, it’s a problem that tears apart families, and even whole communities. It’s important to remain open-minded when deciding what type of treatment is appropriate (or inappropriate) for each individual.
–
 Andrew Huhn is a 4th year PhD candidate in the Neuroscience Graduate Program. He works with Dr. Scott Bunce studying opiate addiction. Andrew enjoys ping pong, ballroom dance, music, and reading.
Andrew Huhn is a 4th year PhD candidate in the Neuroscience Graduate Program. He works with Dr. Scott Bunce studying opiate addiction. Andrew enjoys ping pong, ballroom dance, music, and reading.

Interesting read, it’s a similar discussion as that on the benefits of Methadone and Suboxone. Personally, I’m for whatever works for the individual and I’ve seen huge success as an Addiction Counsellor with heavy IV opiate users getting clean and staying that way after trying every other method possible and finally turning to Medication Assisted Treatment (MAT). I agree that MAT should be combined with therapy, however the amount of time someone remains in MAT is dependent on the amount and type of drug they were using, how long they used for, etc. so some people do need to be on it for several years and slowly taper off.
On another note, while 12-step groups work really well for some people success rates are actually quite low, specifically among youth who use opiates. I would say that evidence-based recovery groups like SMART Recovery work better to change actual addictive behaviours and 12-steps can be great as a spiritual compliment to such groups that are based on science. I’ll probably get a lot of backlash from dedicated 12-step folks for saying that, and again I’m for whatever works, but the science speaks for itself.