by: Katie Kimbark
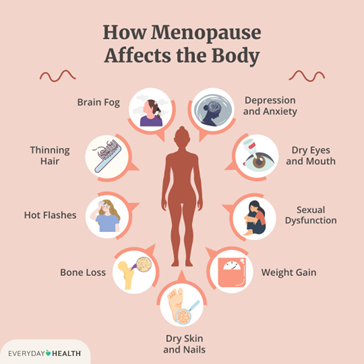
The term “menopause” was first described in the early 1800s by French scientist Charles Pierre Louis de Gardanne.1,2 Despite its descriptions in the preceding millennia, he was the first to designate menopause as a medical phenomenon, distinct from any other stage in a woman’s life. Although women are often attuned to the changes in their menstrual cycles that accompany the menopausal transition, the physical, mental, and emotional effects still take many by surprise. The thousands of testimonies shared by postmenopausal women highlight the heterogeneity of this experience, bringing with it feelings of loneliness in their struggles. This loneliness is further exacerbated by a limited number of effective therapies for the often-burdensome symptoms (Figure 1). Throughout this article, I hope to help explain the biological basis of menopause and related metabolic changes, highlighting some of the most concerning side effects from a public health perspective. From this, I hope you’re able to appreciate the need for more research regarding women’s health, and more conversations to provide a sense of community and hope to women grappling with this “normal” age-related experience.
What is menopause?
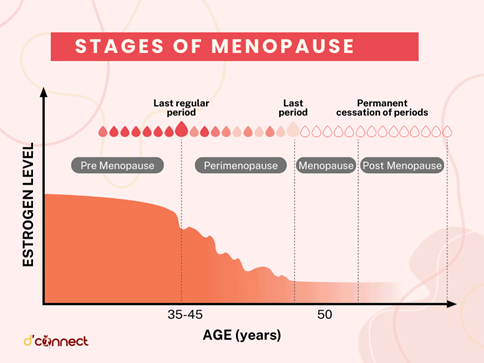
The ovaries, one of the primary female sex organs, is largely comprised of follicular cells which give rise to the eggs released during ovulation each month. Females are born with a fixed number of egg-producing follicles, meaning they have an internal clock dictating their fertility throughout their life. As women age, the quality and quantity of their eggs gradually decrease until they reach full reproductive senescence in menopause. This occurs around age 50, with menopause defined by the absence of a menstrual cycle for a full year.3 Menopause is also marked by a decline in estrogen, the primary female sex hormone produced by ovarian follicles (Figure 2). Some of the most common symptoms associated with the menopausal transition (hot flashes, sleep problems, cognitive and behavioral shifts, and metabolic changes, etc.) are attributed to this loss of estrogen (Figure 1). From this perspective, menopause-related symptoms seem pretty cut-and-dry: you lose estrogen and then start to have hot flashes. The central role of estrogen loss in the menopausal transition is supported by the fact that hormone replacement therapy (HRT) proves effective for many women struggling with these traditional symptoms. However, metabolic changes that come with the menopausal transition are more complex with less clear-cut remedies.
Metabolic changes in menopause – implications of estrogen and beyond
Some of the most burdensome and concerning symptoms of menopause are weight gain and metabolic disturbances, as postmenopausal women are at a three times higher risk of obesity and metabolic syndrome.4 Women often report feeling as if their body shifted overnight despite no changes in their diet or exercise routines. Interestingly, animal models of menopause mimic these sudden changes in body composition and have helped us to better understand the underlying mechanism of this shift. In premenopausal women, estrogen plays a major role in modulating body composition by activating brain regions involved in energy balance to reduce feeding behavior and promote energy usage.5 Estrogen also dictates subcutaneous fat deposition in women. Subcutaneous fat is more metabolically favorable than abdominal (visceral) fat that instead contributes to obesity-related complications, such as metabolic syndrome 6. Upon menopause, women exhibit a shift in the way their body stores fat, with an increase in visceral fat with reduced metabolically-favorable subcutaneous fat, similar to what is seen in men.5 Animal models show similar changes, with “postmenopausal” females displaying increases in feeding and adiposity and decreases in metabolic rate, activity, and lean muscle mass.7 Muscle is an important mediator of energy balance, naturally increasing basal metabolic rate and reducing fat deposition throughout the body. While loss of muscle mass occurs chronologically with aging, women exhibit a more sudden loss following menopause, exacerbating changes in metabolism and energy balance. More recent studies have provided evidence that postmenopausal women actually have increased protein requirements but overall reduced energy needs. Specifically, baseline protein requirements for women increase from 0.8 grams per kilogram of body weight per day to between 1.0 and 1.2 (a drastic difference, as the majority of women already struggle to meet the prior minimum recommendations).8 These data highlight why the changes in body composition occur independent of any lifestyle changes.9
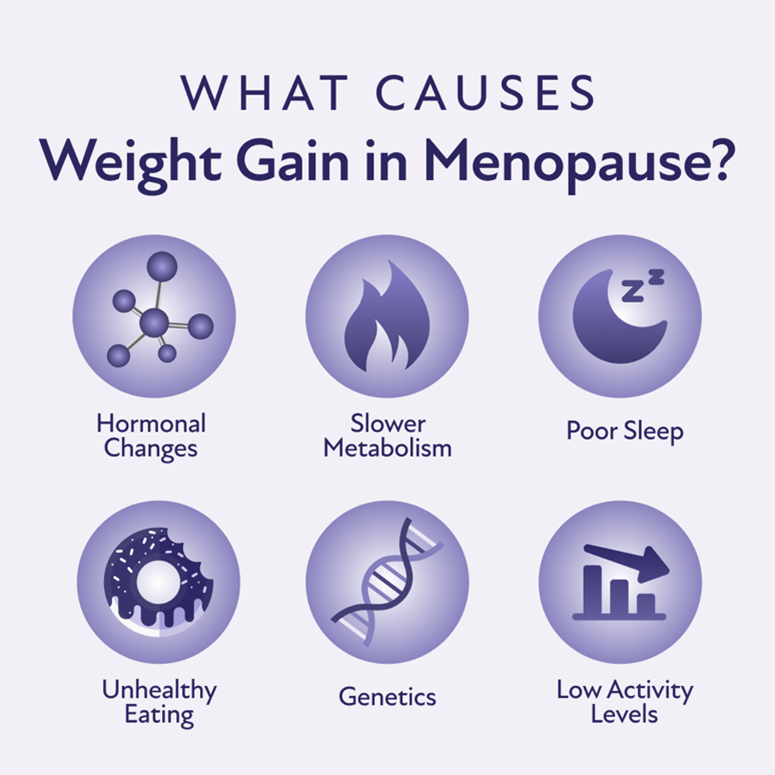
Although menopause causes internal changes in estrogen levels and metabolism, external lifestyle modifications can still minimize menopausal symptoms. Even though hormonal replacement therapy (HRT) proves effective for symptom management for many women, these treatments are not realistic or effective options for all. Safety concerns regarding correlations between HRT and breast cancer risk mean that many women are ineligible for these therapies.10 Further, the connections between menopause and obesity are two sided. Not only do postmenopausal women exhibit an increased risk of obesity, but obese postmenopausal women also display reduced responsiveness to HRT, at only 8% compared to 88% of non-obese women.11 Despite the direct involvement of estrogen in energy balance, obesity is a highly heterogeneous disease with many contributory factors (Figure 3). As such, the effects of HRT on weight management and metabolic outcomes are conflicting, and lifestyle modifications currently serve as the best therapeutic approach.12 Beyond increasing protein intake, exercise is important to conserve muscle mass and minimize negative changes in body composition. Resistance training directly increases lean mass, thus increasing metabolism directly, and also promotes bone health and alleviates some vascular symptoms.13 High-intensity interval training (HIIT) can also prevent menopause-related muscle loss and adiposity while being adaptable to women of varying fitness levels.14 However, it’s important to note that modifications to diet and exercise are not a “one-size-fits-all” policy, and it may take time to figure out what regiments work best for you and your body. Regardless, there is a clear need to deepen our understanding of menopause-related changes in body composition and metabolic processes. A better grasp of the underlying mechanisms is necessary for the development of more effective strategies for improving health and well-being during menopause and beyond.
TL:DR
- Menopause is characterized by the loss of estrogen-producing ovarian cells in middle-aged women.
- Menopause-related metabolic changes are complex and lack substantial therapeutic options outside of lifestyle modifications.
Reference
1. Downham Moore AM. Crises, Critical Ages, and the ‘Invention’ of la Ménopause, c.1770–1812. In: Downham Moore AM, ed. The French Invention of Menopause and the Medicalisation of Women’s Ageing: A History. Oxford University Press; 2022:0. doi:10.1093/oso/9780192842916.003.0004
2. Baber RJ, Wright J. A brief history of the International Menopause Society. Climacteric. 2017;20(2):85-90. doi:10.1080/13697137.2017.1270570
3. Davis SR, Pinkerton J, Santoro N, Simoncini T. Menopause—Biology, consequences, supportive care, and therapeutic options. Cell. 2023;186(19):4038-4058. doi:10.1016/j.cell.2023.08.016
4. Kozakowski J, Gietka-Czernel M, Leszczyńska D, Majos A. Obesity in menopause – our negligence or an unfortunate inevitability? Przegla̜d Menopauzalny = Menopause Review. 2017;16(2):61. doi:10.5114/pm.2017.68594
5. Mauvais-Jarvis F, Clegg DJ, Hevener AL. The Role of Estrogens in Control of Energy Balance and Glucose Homeostasis. Endocrine Reviews. 2013;34(3):309. doi:10.1210/er.2012-1055
6. Booth AD, Magnuson AM, Fouts J, et al. Subcutaneous adipose tissue accumulation protects systemic glucose tolerance and muscle metabolism. Adipocyte. 2018;7(4):261-272. doi:10.1080/21623945.2018.1525252
7. Zidon TM, Padilla J, Fritsche KL, et al. Effects of ERβ and ERα on OVX-induced changes in adiposity and insulin resistance. J Endocrinol. 2020;245(1):165-178. doi:10.1530/JOE-19-0321
8. Black KE, Matkin-Hussey P. The Impact of Protein in Post-Menopausal Women on Muscle Mass and Strength: A Narrative Review. Physiologia. 2024;4(3):266-285. doi:10.3390/physiologia4030016
9. Simpson SJ, Raubenheimer D, Black KI, Conigrave AD. Weight gain during the menopause transition: Evidence for a mechanism dependent on protein leverage. BJOG: An International Journal of Obstetrics & Gynaecology. 2023;130(1):4-10. doi:10.1111/1471-0528.17290
10. Harper-Harrison G, Carlson K, Shanahan MM. Hormone Replacement Therapy. In: StatPearls. StatPearls Publishing; 2024. Accessed November 20, 2024. http://www.ncbi.nlm.nih.gov/books/NBK493191/
11. Pershad A. Self-reported efficacy of hormone therapy and symptom burden in menopausal patients with obesity. Presented at: Annual Meeting of the Menopause Society; September 27, 2023; Philadelphia.
12. Lovre D, Lindsey SH, Mauvais-Jarvis F. Effect of menopausal hormone therapy on components of the metabolic syndrome. Ther Adv Cardiovasc Dis. 2017;11(1):33-43. doi:10.1177/1753944716649358
13. Capel-Alcaraz AM, García-López H, Castro-Sánchez AM, Fernández-Sánchez M, Lara-Palomo IC. The Efficacy of Strength Exercises for Reducing the Symptoms of Menopause: A Systematic Review. Journal of Clinical Medicine. 2023;12(2):548. doi:10.3390/jcm12020548
14. Hubbard EF, Mashouri P, Pyle WG, Power GA. The effect of gradual ovarian failure on dynamic muscle function and the role of high-intensity interval training on mitigating impairments. American Journal of Physiology-Cell Physiology. 2023;325(4):C1031-C1045. doi:10.1152/ajpcell.00318.2023

Fascinating read! This exploration of menopause and its connection to hormones, health, and aging provides valuable insights into an often misunderstood topic. Thanks for shedding light on this!