By Stephen Matthews
There’s a lot of misconception surrounding inflammatory bowel disease (IBD). I find most people have heard of it, but few people understand what it is or what patients with IBD deal with. As a researcher working on IBD, I thought I could take some time to explain some of the complications, treatments and definitions of IBD.
To appreciate the disease, I need to cover how the gastrointestinal (GI) tract is structured, first. As the core component of the digestive system, the GI tract forms a continuous tube that encompasses all connected organs between the mouth and the anus, and is largely responsible for digesting food, extracting nutrients and expelling solid waste matter. Each section of the human GI tract fills its own role, and can be further broken down into smaller components, but at minimum is composed of the esophagus, stomach, small and large intestines, and the rectum. An important and sometimes underappreciated aspect of this structure is that even though food you eat is inside you, it is still not really inside your body. A simplistic way to visualize your body is by imagining a donut, where the donut hole is the GI, the outside of the donut is your skin, and the inside of your body is the inside of the donut (Figure 1). Importantly, the connection between the skin and GI is uninterrupted, forming a constant layer of protection across all sides of the donut. Stretching this donut into a cylinder better represents this system, where the food you eat moves through the donut hole/GI but does not enter your body.
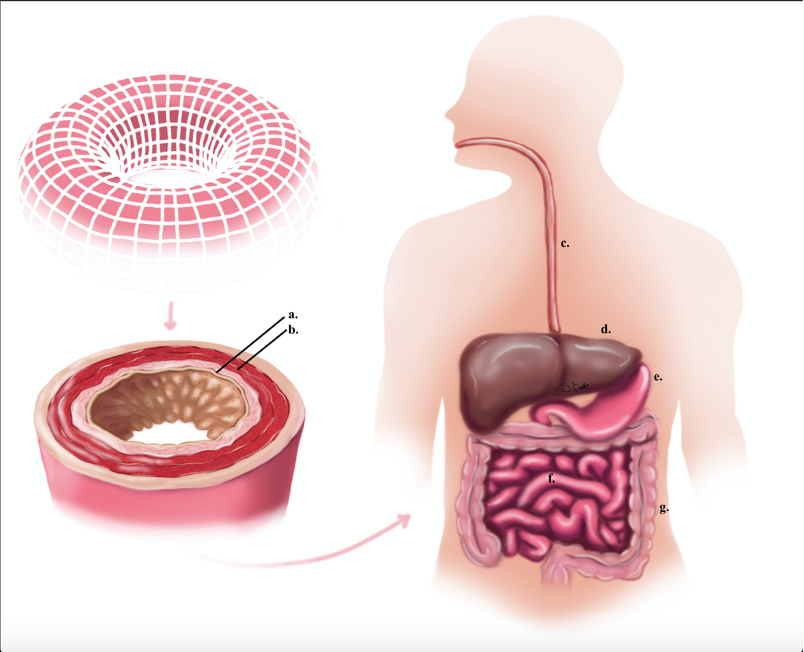
If you were to fall and scrape your knee, your skin would be damaged, this triggers an immediate immune response to orchestrate the healing process. Similarly, the immune response is also activated when your intestinal epithelium is damaged. This immune response is critical when the GI is damaged, because the intestines are host to a vast array of commensal bacteria, termed the microbiota. However, due to the importance of nutrient absorption by the GI, it must function as a selective barrier to keep out bacteria while also absorbing nutrients. Structurally, the small intestine is covered in fingerlike projections called “villi.” Much like the crevices of a paper towel, these villi drastically increase the surface area of the small intestine to help nutrient absorption. This absorptive, epithelial layer is wrapped by blood vessels and muscle layers that help distribute absorbed nutrients, and also contract the intestines to push food through it. Your large intestine lacks these villi and focus on water absorption, but otherwise is structured the same. All this is to say the GI is a specialized and sensitive system that performs a critical, multipurpose role in protection and nutrient absorption. When this system is damaged, or the immune system is over-activated, as it is in the chronic inflammation of IBD, the consequences can be dire and life-threatening, ranging from dehydration and malnutrition to anemia, intestinal blockages, and perforations of the bowel wall.
IBD is a recrudescent chronic inflammatory disease of the gastrointestinal tract and can develop in adults and children alike. According to the Crohn’s and Colitis Foundation of America (CCFA), IBD affects 1.6 million people in the USA, gaining about 70,000 additional cases a year. The severity and extent of inflammation can range from asymptomatic, to crippling pain that drastically affects the life of the patient. It is subcategorized into two main subtypes, Crohn’s disease (CD) and ulcerative colitis (UC), which have a distinct yet overlapping presentation in patients. UC presents as inflammation limited to the epithelial layer, beginning at the rectum and proximally extends, at maximum, to include the entire large intestines. Inflammation can be visualized in the large intestine as mild redness, or as characteristic ulcerations. CD differs from UC in that it presents as a non-contiguous inflammation and can occur sporadically anywhere along the GI tract, from the esophagus through to the anus. CD involves “transmural inflammation” which can spread to the muscle layers and is not limited only to the mucosa. This transmural inflammation can lead to thickening of the bowel wall, resulting in a “cobblestone” pattern of coalesced ulcerations: ulcers that are so close and frequent that they meld into a mass. While both CD and UC have high propensity for complications, CD is frequently met with more macroscopic complications due to its transmural inflammation. One such complication is a fistula, where inflammation causes the inflamed portion of the GI to fuse to another part of the body. There are also several non-intestinal manifestations that can occur, as both CD and UC exhibit hyper-activation of the immune system. These concomitant byproducts can include joint pain, organ damage, and lesions in other places of the body, while also increasing the likelihood to develop colorectal cancer. Suffice it to say, having IBD is more complicated than “just pain in the GI,” and can drastically influence one’s quality of life.
The cause of IBD is unknown and accepted to result from exposure to environmental factors in genetically susceptible individuals. However, IBD development is not a simple cause-effect relationship. Each risk factor is interdependent, and carries a different level of impact in IBD development, making the study of IBD very challenging. When a perfect storm of environmental and genetic factors converge in a person, IBD can develop. By virtue of being an inflammatory disease, there is a well-established impairment of the immune system, whose overactivation stems from several potential mechanisms. Some risk factors distinctly influence UC or CD, while others are associated with the development of both, but all risk factors can be classified at the simplest level into “host factors” or “environmental factors.” Environmental risk factors are controllable, like smoking status, diet, medications, geographic location, and the GI microbiome. Host factors, by comparison, are pre-determined genetically (ethnicity, family history, and genetic mutations) and function as the foundation for disease pathogenesis.
There are several treatment regimens available to help patients manage their disease, though there is no cure for IBD. The goal of therapy is two-fold: to introduce remission, and maintain remission. Due to the complexity of the disease, patients will frequently require several different mediations to induce and/or maintain remission over their lifetime. The method of treatment is determined through classification of the disease extent and severity, and utilizes several drugs. Most treatments are oriented towards repressing the immune response so the GI can heal itself, and include aminosalicylates, corticosteroids, and immunomodulatory agents or “biologics.” Biologics are the newest addition to IBD therapy repertoire and are laboratory-created therapies that, for IBD, are designed to block or reduce the presence of inflammatory proteins, resulting in a repression of this characteristic inflammation. While this generally helps the patient’s body repair itself, any kind of immunomodulation leaves a patient more susceptible to other infections that normally pose a low health risk. During the current COVID-19 pandemic, SARS-CoV-2 is a very real danger to patients on any immunomodulatory medications (again illustrating how important mask and distancing mandates are). Due to the complexities of each disease, the drug response differs between CD and UC, and not all medications effectively treat both types of disease, or work in all patients. In these instances, surgery may be required to manage the disease. While this helps the patient with the symptoms of IBD, it will alter their quality of life, present new challenges or additional complications, and may only be a temporary reprieve.
We often hear about bowel diseases and disorders on television advertisements or social media, but may never understand what they really are. Hopefully upon reading this article you have a better understanding of IBD, and an appreciation for the difficulties faced by those who have it. Each person with IBD (or similar diseases like Celiac disease or irritable bowel syndrome (IBS)) leads a complex life with a great deal of stress and maintenance. Therefore, it is important to recognize the complexity and seriousness of these diseases to fully appreciate the lives of those affected.
References:
Szmulowicz U.M., Hull T.L. (2011) Colonic Physiology. In: Beck D.E., Roberts P.L., Saclarides T.J., Senagore A.J., Stamos M.J., Wexner S.D. (eds) The ASCRS Textbook of Colon and Rectal Surgery. Springer, New York, NY. Pg. 23-39.
Koltun W.A. (2011) IBD: Diagnosis and Evaluation. In: Beck D.E., Roberts P.L., Saclarides T.J., Senagore A.J., Stamos M.J., Wexner S.D. (eds) The ASCRS Textbook of Colon and Rectal Surgery. Springer, New York, NY. Pg. 449-462.
Sands B.E. (2011) IBD: Medical Management. In: Beck D.E., Roberts P.L., Saclarides T.J., Senagore A.J., Stamos M.J., Wexner S.D. (eds) The ASCRS Textbook of Colon and Rectal Surgery. Springer, New York, NY. Pg. 463-478.
https://www.crohnscolitisfoundation.org/sites/default/files/2019-02/Updated%20IBD%20Factbook.pdf
