By Jillian Carmichael, PhD
By now, you’d need to be living under a rock to have not heard about the new coronavirus. COVID-19 was officially declared a pandemic by the WHO (World Health Organization) on Wednesday. As of Friday, March 13, there are more than 1600 diagnosed COVID-19 cases in the US and more than 118,000 cases worldwide. However, the numbers are constantly changing so by the time this is published, this reporting will be obsolete.
In times like these, there are many “hot takes” in the media about what you should do in response to the pandemic. This is not one of those posts. Instead, I’m opting for some old-fashioned biology education to help you better understand what’s going on from a scientist’s perspective. Perhaps you can guess what this means… it’s time for definitions! Here’s some virology terminology needed to better understand this pandemic:
SARS-CoV-2—This stands for “severe upper respiratory syndrome coronavirus 2.” This is the actual name of the virus, as determined by the ICTV (the International Committee on Taxonomy of Viruses). SARS-CoV-2 belongs to the coronavirus family and has an RNA genome of about 30,000 bp.
COVID-19—This means “coronavirus disease 2019” and is the disease caused by the virus, SARS-CoV-2. While it may seem weird, viruses and the diseases they cause can have different names.
PCR—This is an acronym for “polymerase chain reaction.” PCR is a common molecular biology technique that scientists can use to detect specific pieces of DNA. To determine if there is coronavirus RNA present in a sample (coronaviruses have RNA genomes), scientists are using a technique called RT-qPCR. They first take the patient sample and convert any potential viral RNA to DNA. Next, they use small pieces of DNA (primers) that are highly specific to SARS-CoV2 to amplify it. This means that if there was SARS-CoV2 RNA in the patient sample, scientists will be able to specifically detect and quantify it with this PCR tool. For now, this is how scientists are confirming coronavirus cases. It takes time, expertise, and money (and primers that are designed correctly).
Viral load—This term refers to how much infectious virus is present in a sample. While PCR can tell us if there is SARS-CoV2 RNA in a sample, it cannot tell us how much virus there is. Sometimes scientists and doctors will use a phrase like “high viral load” to indicate that a patient has a large amount of infectious virus in their sample. Depending on the type of virus, scientists have different techniques to measure how much virus there is in a sample or experiment. After all, science is nothing without quantitation! For SARS-CoV2, scientists use what is called a plaque assay to calculate how much infectious virus they have. This involves growing the virus in cell culture, seeing which cells die from infection, and some basic algebra. At the end, viral load is typically reported as the amount of infectious virus per volume.
Host—In terms of virology, a host is the species infected by a particular virus. In order to make more of themselves, viruses must go inside of a host cell and hijack its machinery. A host can be anything from bacteria, to plants, to animals, to humans. Most viruses are limited to specific hosts. What this means is that human viruses infect humans and not plants. Viruses that infect bacteria, don’t make humans sick. The scientific term for this is “host specificity.” However, sometimes viruses that infect animals can also make humans sick (see below).
Zoonotic—Zoonotic infections occur when a virus, bacteria, or parasite that normally infects animals can also infect humans and make us sick. We call this “jumping species” since the pathogen moves from one species to another. There are several ways that pathogens can jump from animals to humans including insect bites (Dengue virus, malaria etc.), exposure to animal droppings (Nipah virus), and close contact. It is currently believed that SARS-CoV2 originated in bats and jumped species into humans. There may also be an intermediate host—this means that another animal could have served as the link to move SARS-CoV2 from bats to humans. Some zoonotic infections have been around for a long time, like malaria. Others, like SARS-CoV2 are new to humans—we call these emerging pathogens.
Vector—A vector is an agent that transmits a pathogenic infection to someone else. In terms of zoonotic infections, vectors can be animals and mosquitoes. For many human infections, humans can act as vectors, spreading the disease to other people. Unfortunately for the COVID19 pandemic, humans are effective vectors. This results in human-to-human transmission of SARS-CoV2.
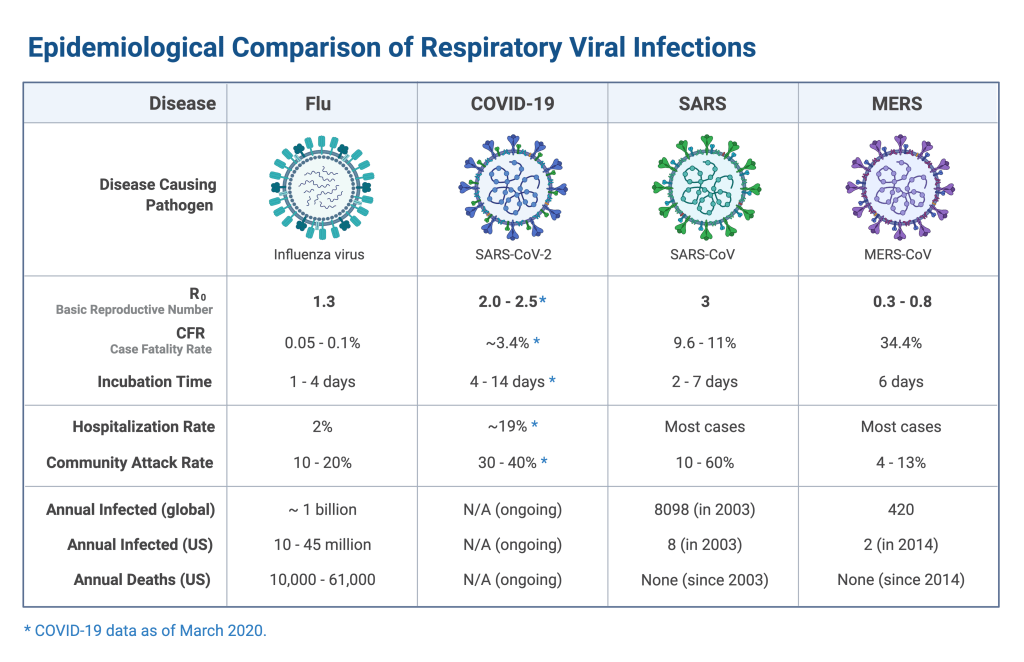
R0 (pronounced R-naught)—The R0 is the basic reproductive number of the virus. It is an estimate of how many people one sick person will infect. The higher the R0, the more contagious the virus. For example, measles virus is the most contagious human virus and has an R0 of 12-18. Pre-vaccination, this means that one person infected with measles would on average infect 12-18 new people. Seasonal influenza has an R0 of 1-2. SARS-CoV2 is thought to have an R0 between 2-3, but these numbers will change as time goes on and we gather more data. It’s important to remember that the R0 is an estimate, not a hard fact.
Case Fatality Rate (CFR)—The Case Fatality Rate is how many deaths a pathogen causes out of the total number of people infected. It’s expressed as a percentage. For now, the CFR for COVID-19 is somewhere between 0.8-3%. This means that for every 1000 people infected with SARS-CoV2, between 8 and 30 people will die. HOWEVER, the CFR directly depends on diagnostics. The CFR will be falsely high if we aren’t detecting mild or asymptomatic infections. South Korea has been diligent in testing people for SARS-CoV2. Their estimated CFR is lower (about 0.8%) than in places with limited viral testing. The CFR can also vary with medical interventions. In places where there are lots of resources and doctors to treat COVID-19, the CFR will likely be lower. However, in places where resources are limited, the CFR will be higher. This is what’s happening in Italy as they are overwhelmed with cases and are currently reporting a CFR of 6%. Count on the CFR to continue changing (hopefully decreasing) as we gain a better understanding of just how many people are infected with SARS-Cov2.
“Flattening the curve”—Thanks to public health officials, the idea of “flattening the curve” has quickly entered everyday conversation. In the case of COVID-19, to “flatten the curve” means to try and reduce the number of people contracting the virus all at once. By limiting ways for the virus to spread, we can reduce burdens on our healthcare systems so they don’t become completely overwhelmed with sick patients. This could mean canceling big events, limiting travel, and self-quarantine if necessary. The technical term public health officials use for this is social distancing. This won’t stop all virus spread, but it will slow it down, so that our healthcare system can have the time and resources to respond. The illustration below is an excellent visual representation of flattening the curve.

I wrote this because I love science communication and there is often a gap between what scientists and academics discuss and the information communicated to non-scientists. Remember, we should not let fear of the unknown control our actions and thoughts. Rather, we must make scientifically-informed decisions and fund scientific research!
Stay curious,
Jillian Carmichael, PhD
2019 graduate of the Penn State COM BMS program
Virologist & Postdoctoral Fellow at the Icahn School of Medicine at Mount Sinai
Twitter: @ViralCarmichael
Sources
- https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200311-sitrep-51-covid-19.pdf?sfvrsn=1ba62e57_6
- https://www.nejm.org/doi/full/10.1056/NEJMoa2002032
- https://www.cdc.gov/coronavirus/2019-ncov/about/index.html
- https://jamanetwork.com/journals/jama/fullarticle/2762997
- https://www.sciencedirect.com/science/article/pii/S0140673620305572?via%3Dihub
- https://www.ncbi.nlm.nih.gov/books/NBK554776/
- https://www.thelancet.com/action/showPdf?pii=S0140-6736%2820%2930627-9
- https://www.biorxiv.org/content/10.1101/2020.03.02.972935v1.full.pdf

This was very helpful because I am only 10 and I want to be a virologist when I grow up.