By Rachel Kang
Introduction
The Castro District, known locally as The Castro, was one of the first gay neighborhoods in the United States. It transformed from a predominately working-class neighborhood to a hotspot of LGBTQ+ activism in the 1970s. Gay men flooded the streets, dancing, smiling, and proud to be who they were and to love who they wanted. For these men, the neighborhood was a haven from an otherwise homophobic country. Here at the Castro, many gay men felt free.
This dream quickly ended as the people around them (lovers, spouses, brothers) began to die and no one understood why.
Today, we know that many of these men were infected by human immunodeficiency virus (HIV). When left untreated, an HIV infection will develop into acquired immunodeficiency syndrome (AIDS), the most advanced stage of HIV1. Soon after the first cases of HIV/AIDS emerged in the US, the disease rapidly grew into an outbreak where people, particularly gay men and other underprivileged groups, died without cause or reason. A stigma grew where people used HIV/AIDS to fear, hate, or ostracize those with the disease or those most impacted by it. HIV/AIDS is a scary, life-changing diagnosis, and the lack of information surrounding the disease inflated its horror (Figure 1). However, science has come a long way since the 1970s, and while there is still no cure, people are more equipped to deal with an HIV+ diagnosis than ever before.

Biology of HIV/AIDS
A virus is an infectious microbe that is reliant on a host cell to build more copies of itself. Viruses are comprised of genetic material (DNA or RNA) and proteins, which it uses to attach itself to a cell and make it into a virus-producing machine. Once multiple copies of the virus are assembled, the cell ruptures and the virus particles, also known as virions, are released to make more copies of the virus2,3.
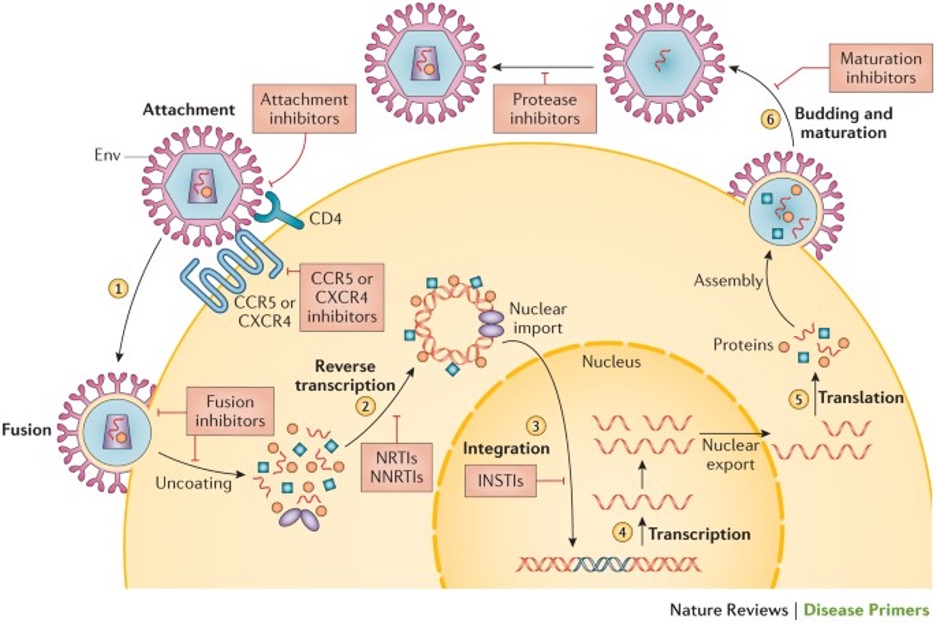
What makes HIV unique is that it is a retrovirus: it can integrate its genetic material into the host’s DNA (Figure 2)4. Rather than just hijacking the cell to produce more copies, the cell transforms into an HIV producing factory. Additionally, because HIV’s genetic material is RNA, it must undergo reverse transcription to become DNA before integrating into the host’s genome. However, reverse transcription is an error-prone process; HIV is said to have 5 to 10 errors per round of replication5,6. As a result, HIV generates numerous mutations which each undergo natural selection. Unfortunately, these mutations can promote treatment resistance. For example, one treatment may cause one strain of HIV to die out; however, that still leaves several other HIV strains available to continue infecting other cells. If left untreated, more and more strains of HIV are created, making the disease increasingly treatment resistant.
Medical management of the HIV virus is crucial to maintain a healthy immune system. HIV preferentially infects a type of white blood cell known as CD4 cells7. These CD4 cells (also known as helper T-cells) release molecules that tell other immune cells like B-cells or cytotoxic T-cells to kill infected cells. When HIV infects a CD4 cell, the virus ruptures the cell to release the newly formed virus particles and kills the host cell in the process. As the replication process repeats in other CD4 cells, the population of CD4 cells decreases. In response to the infection, the immune system signals to the body to produce more CD4 cells. However, due to the exponential growth of virus particles, HIV tends to kill more CD4 cells than the body can produce. Without enough CD4 cells, the immune system is weakened, and the body becomes unable to fight off any infection.
People infected with HIV initially experience flu-like symptoms such as fatigue, sore throat, swollen lymph nodes and joint pain. As the viral load, the amount of virus particles in your body, increases, the infection advances to include symptoms such as oral yeast infections (thrush), white patches on your tongue (oral hairy leukoplakia), and pain or weakness in the hands or feet (peripheral neuropathy)8. Without intervention or treatment, an HIV infection can further advance into AIDS where a patient becomes predisposed to rare or unusual diseases not seen in healthy populations. In fact, the discovery of AIDS in the United States came to attention when populations of gay men began developing pneumonia or a type of skin cancer often seen in immune-compromised populations.
Who is most affected by HIV/AIDS?
According to the World Health Organization (WHO), in 2022 an estimated 39 million people are living with HIV worldwide, with 1.3 million new cases in just the last year. In different parts of the world, HIV affects different adult populations. In sub-Saharan Africa, over half of all HIV infections are women9. In the United States, the majority of new HIV infections were found to be among men having sex with men10.
HIV is a sexually transmitted infection that spreads from person to person through any kind of sexual activity. The HIV epidemic in the US occurred during one of the most active moments of LGBTQ+ political activism in the 1970s. However, as the epidemic grew, and more and more gay men began dying from the then unknown infection, people began attributing the disease as a punishment for their “unsavory” behavior.
Viruses and infections are not sentient and cannot exact judgement of people deemed “lesser” in society’s eyes. Anyone can develop HIV/AIDS if exposed to the virus. Homosexual men, during this time of sexual freedom, could explore new experiences they might have missed while being in the closet. Furthermore, there was a distinct lack of sexual education beyond abstinence and there was no coverage on safe non-heterosexual sex11. It was no moral failing of these men that gave them HIV/AIDS; it was instead, the systemic failure of society that provided no support for these victims as they died in their lovers’ arms (Figure 3).
Why No One Cared
Until the 1960s, homosexuality was not discussed among the public, and surely not in the presence of prestigious researchers. Though LBGTQ+ activism was at an all-time high, it was being pushed back in equal force by conservative leaders such as Anita Bryant. As men began to die in The Castro and in the streets of New York City, there became “a strong view that some people are worthier of being kept alive than others12.” With United States health research being underfunded and researchers themselves having their own biases, HIV/AIDS was unfortunately put to the side until famous actor Rock Hudson became the first high-profile fatality from AIDS.
It soon became obvious that AIDS did not just affect gay men, and by not providing care and support for them, you are essentially depriving resources to the larger community as well. It is a tragedy that these men died, and society turned their backs on them for religious beliefs, personal biases, or simple apathy to their suffering. As more diseases like monkeypox pop up that seem to disproportionately affect marginalized groups, it is more important than ever to have diversity in STEM and STEM research to let these people know they are not alone.
TL;DR
- Human immunodeficiency virus (HIV) causes acquired immunodeficiency syndrome (AIDS) if left untreated.
- HIV’s reverse transcription is error-prone and produces many different strains, making the disease difficult to cure.
- For additional reading, check out And the Band Played On: Politics, People and the AIDS Epidemic by Randy Shilts. Highly recommended!
- Get tested! There’s no shame, and it will help prevent future outbreaks of HIV!
References
1. Wattanasirikosone, R., & Modnak, C. (2022). Analysing transmission dynamics of HIV/AIDS with optimal control strategy and its controlled state. Journal of Biological Dynamics, 16(1), 499–527. https://doi.org/10.1080/17513758.2022.2096934
2. Boulant, S., Stanifer, M., & Lozach, P.-Y. (2015). Dynamics of Virus-Receptor Interactions in Virus Binding, Signaling, and Endocytosis. Viruses, 7(6), 2794–2815. https://doi.org/10.3390/v7062747
3. Lozach, P.-Y. (2020). Cell Biology of Viral Infections. Cells, 9(11), 2431. https://doi.org/10.3390/cells9112431
4. Deeks, S. G., Overbaugh, J., Phillips, A., & Buchbinder, S. (2015). HIV infection. Nature Reviews Disease Primers, 1(1), Article 1. https://doi.org/10.1038/nrdp.2015.35
5. Preston, B. D., Poiesz, B. J., & Loeb, L. A. (1988). Fidelity of HIV-1 Reverse Transcriptase. Science, 242(4882), 1168–1171. https://doi.org/10.1126/science.2460924
6. Overbaugh, J., & Bangham, C. R. M. (2001). Selection Forces and Constraints on Retroviral Sequence Variation. Science, 292(5519), 1106–1109. https://doi.org/10.1126/science.1059128
7. Vidya Vijayan, K. K., Karthigeyan, K. P., Tripathi, S. P., & Hanna, L. E. (2017). Pathophysiology of CD4+ T-Cell Depletion in HIV-1 and HIV-2 Infections. Frontiers in Immunology, 8, 580. https://doi.org/10.3389/fimmu.2017.00580
8. Justiz Vaillant, A. A., & Gulick, P. G. (2023). HIV Disease Current Practice. In StatPearls. StatPearls Publishing. http://www.ncbi.nlm.nih.gov/books/NBK534860/
9. Moyo, E., Moyo, P., Murewanhema, G., Mhango, M., Chitungo, I., & Dzinamarira, T. (2023). Key populations and Sub-Saharan Africa’s HIV response. Frontiers in Public Health, 11, 1079990. https://doi.org/10.3389/fpubh.2023.1079990
10. Lansky, A., Brooks, J. T., DiNenno, E., Heffelfinger, J., Hall, H. I., & Mermin, J. (2010). Epidemiology of HIV in the United States. JAIDS Journal of Acquired Immune Deficiency Syndromes, 55, S64. https://doi.org/10.1097/QAI.0b013e3181fbbe15
11. Blair, T. R. (2017). Safe Sex in the 1970s: Community Practitioners on the Eve of AIDS. American Journal of Public Health, 107(6), 872–879. https://doi.org/10.2105/AJPH.2017.303704
12. Grönfors, M., & Stalström, O. (1987). Power, Prestige, Profit: AIDS and the Oppression of Homosexual People. Acta Sociologica, 30(1), 53–66. https://doi.org/10.1177/000169938703000103
